Complication fungique après résection chirurgicale d’un méningiome frontal
Complication fungique après résection chirurgicale d’un méningiome frontal
Introduction
Reconstruction du calvarium après crâniotomie :
- Réimplantation du volet
- Des deux tables
- De la table externe uniquement
- Allogreffes
- Prothèses synthétiques / Métalliques
- PMMA
- La plus courante
- La plus facile d’utilisation
- Intéressante financièrement
- Risques septique ( 13 % chez l’Homme)
Auteur: Dr. S.Libermann. 28-10-2014
Centre Hospitalier Vétérinaire des Cordeliers, 29 avenue du Maréchal Joffre, 77100 Meaux.
E-mail: slibermann@chvcordeliers.com
Cas clinique
Chienne Boxer stérilisée 9,5 ans
Crises convulsives depuis 1 an traitées
(Phénobarbital / Bromure – Crisax ND)
Modification récente du comportement
Apparition d’une anisocorie avec mydriase aréflectique à droite
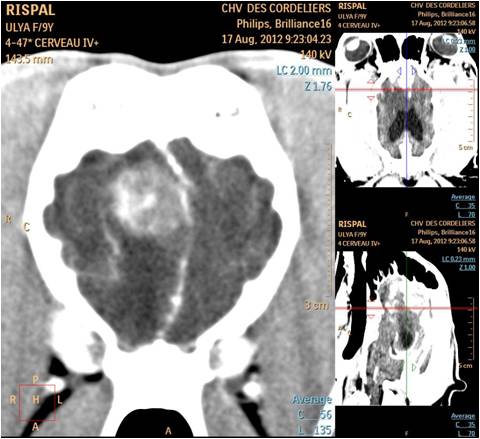
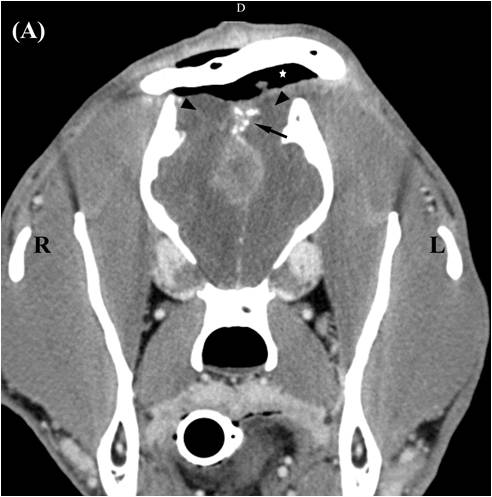
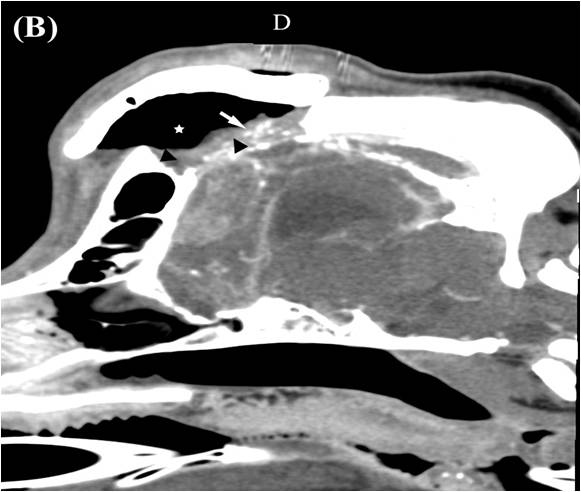
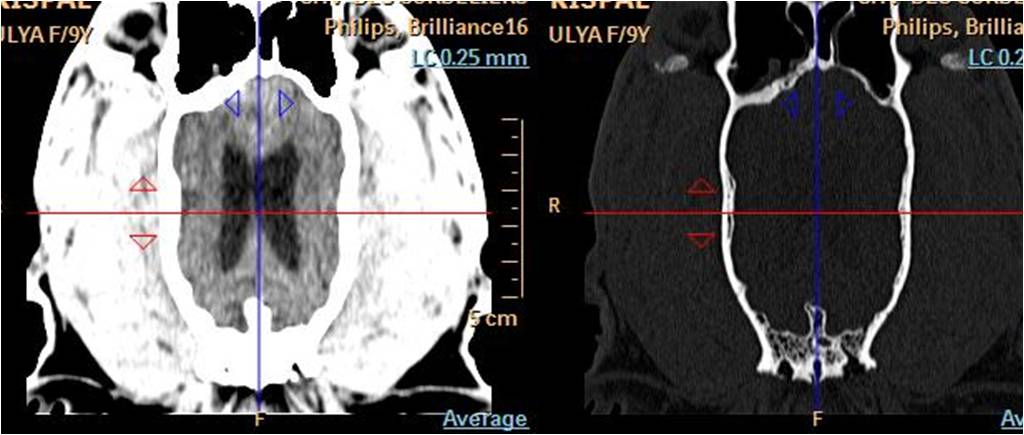
Examen tomodensitométrique
- Aspect compatible avec un méningiome du lobe frontal gauche
- Masse hyperdense, calcifiée
- Rehaussée après injection
- Déviation de la faux
- Réaction osseuse pariétale
Examen du LCS : normal
Traitement chirurgical
- Résection des deux tables du calvarium, ouverture du sinus frontal
- Dissection sous microscope
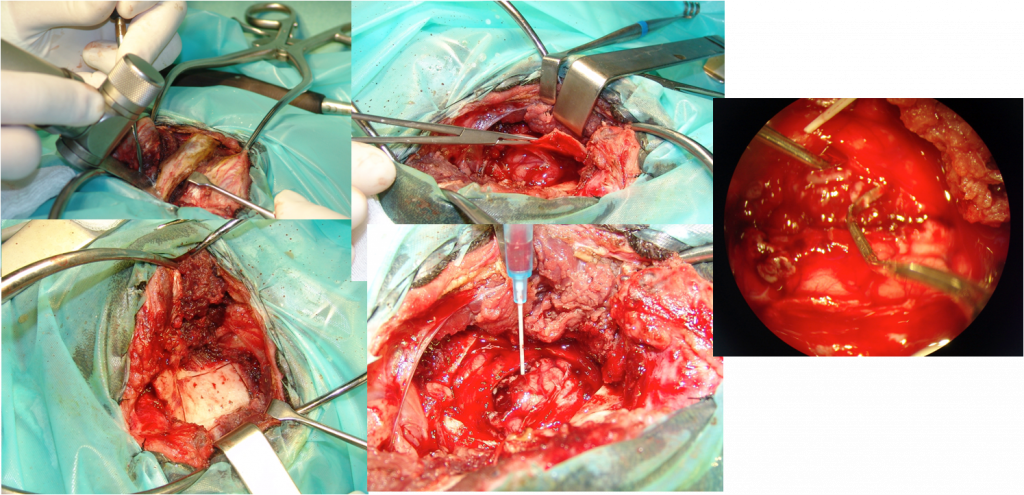
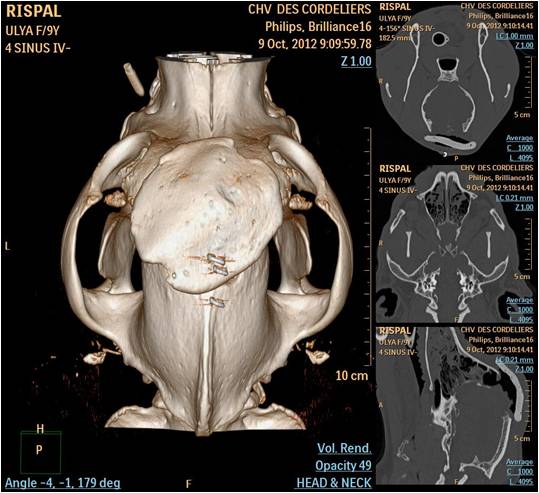
- Mise en place d’une prothèse de PMMA
- Plus large que de défect osseux pour éviter toute pénétration
Suivi
- Post-opératoire immédiat
- Fentanyl (Janssen) bolus 2 µg/kg suivi par 2 µg/kg/h, puis morphine (Morphine chlorhydrate; Aguettant) 200 µg/kg/4h / 48 hours ketamine (Virbac) bolus 500 µg/kg suivi par 500 µg/kg/h for 6 hours.
- Score de Glasgow toutes les 4 heures
- Bolus de Phenobarbital (Gardenal; Sanofis- Aventis France) : 16 mg/kg puis 150 µg/kg/h pendant 48 heures
- Oxygène 18 heures PO
- Post-opératoire après sortie d’hospitalisation
- Confirmation d’un méningiome transitionnel : marges saines
- Phenobarbital : 2 mg/kg/j BID
- Méthyl Prednisolone 1 mg/kg/j BID
- Céphalexine 30 mg/kg/j BID
- Marbofloxacine 4 mg/kg/j SID
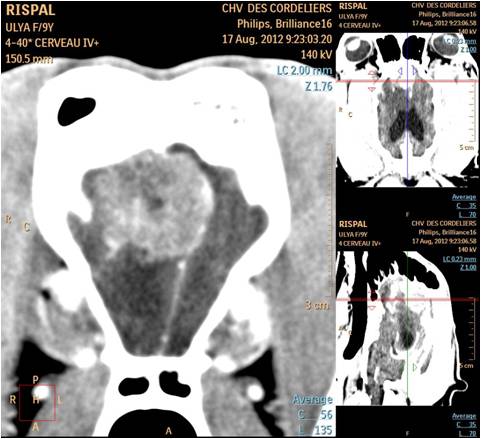
- Post-opératoire + 6 semaines : écoulement nasal ne rétrocédant pas aux traitements anti-infectieux
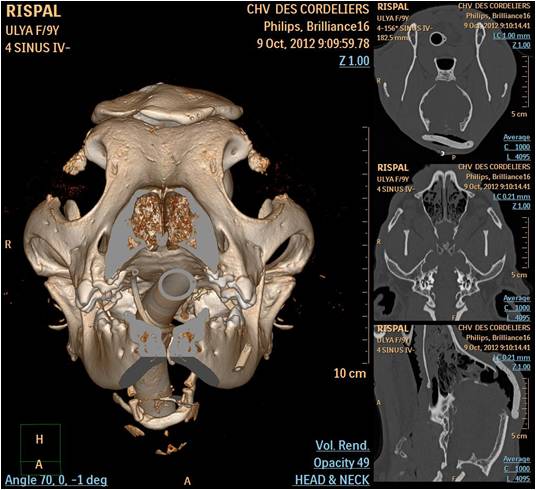
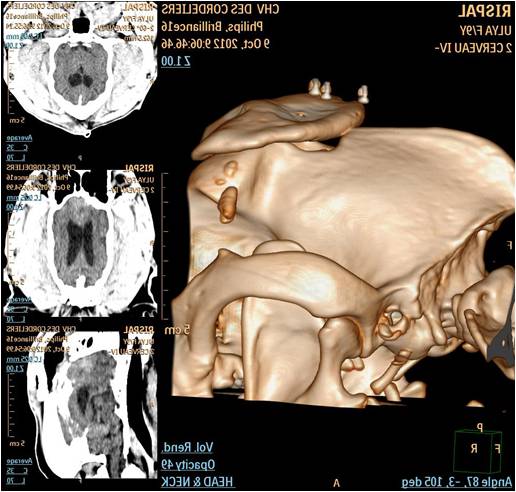
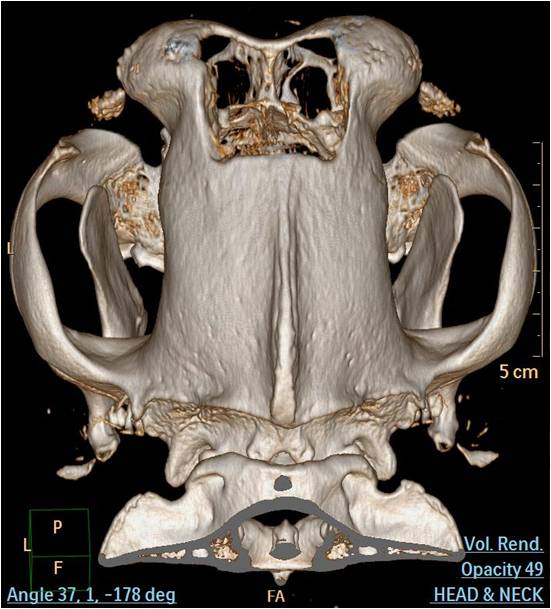
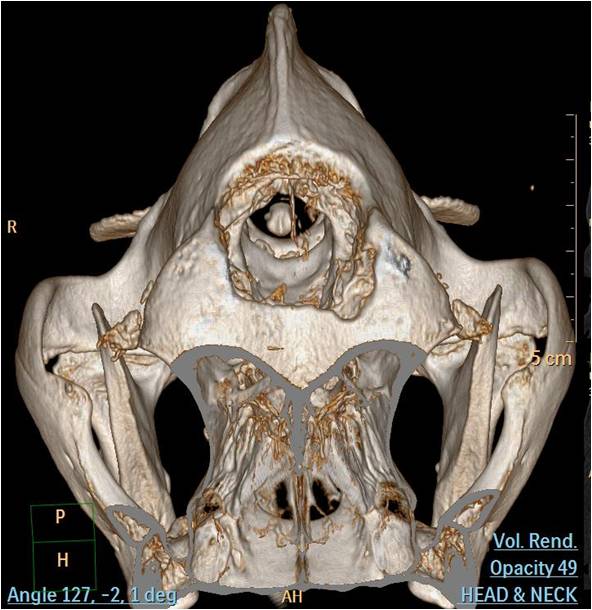
- Scanner
- Prolifération d’un tissu couvrant le défect osseux
- Zones de calcification dans le tissu compatible avec une aspergillose sinusale
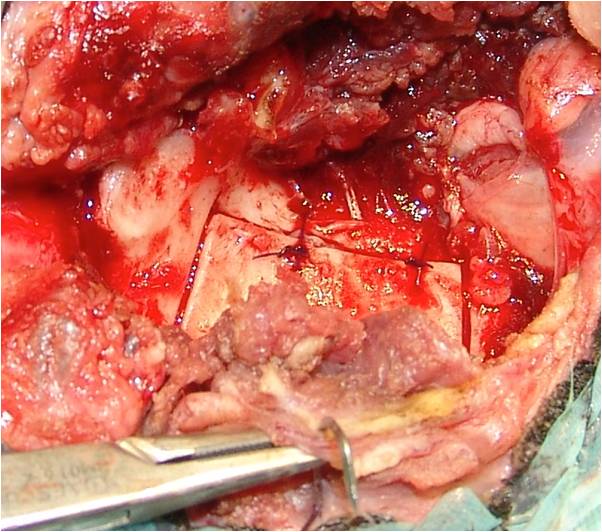
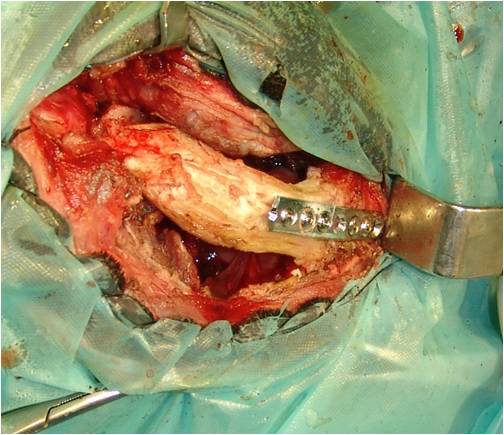
- Résection en bloc du PMMA et confirmation de la colonisation par aspergillus fumigatus
- Un tissus cicatriciel couvre les méninges : laissé sans protection
- Itraconazole 1 mois
- Guérison clinique de la rhinite
- Demande d’euthanasie 9 mois post-opératoire
- Réapparition des crises épileptiformes
- Euthanasie sans examen d’imagerie ou nécropsique
Discution
Utilisation du PMMA
- Risque septique avéré chez l’homme
- En particulier lors d’implantations en contact avec les sinus frontaux
- Uniquement affections bactériennes
- → Premier cas décrit de contamination fungique
Aspergillose chez le chien
- Etiopathogénie mal connue : affection saprophyte
- Facteurs prédisposants documentés :
- Corps étrangers
- Affections dentaires
- Traumatisme facial
Aspergillus présent avant la craniectomie
Ou
Favorisé par le trauma de la craniectomie ?
- Sensibilité du scanner au diagnostic des Aspergilloses sinusales ayant une répercussion clinique : 88 à 92 %
- Mais aucune information sur les animaux porteurs sains
→ Impossible de choisir le type de prothèse en excluant une contamination des sinus par Aspergillus F.
Recommandations ?
- Éviter le PMMA en contact avec les cavités sinusales
- Favoriser une réimplantation de la table externe
- Mais difficile à prélever : finesse osseuse du calvarium sinusal
- Difficultés à séparer les deux tables chez le chien
- Utilisation possible de l’arcade zygomatique par un abord latéral
- Risque d’enfoncement et de lésion cérébrale
- Résection du calvarium nécessaire dans un contexte de chirurgie carcinologique
- Implantation du PMMA
- Modelé sur le calvarium réséqué et implanter dans le défect ?
Ou - Plus large et en sur épaisseur ?
- → Favorisation d’un espace mort, augmentant le risque de sepsis ?
- Modelé sur le calvarium réséqué et implanter dans le défect ?

Conclusion
1er cas décrit de contamination du PMMA par Aspegillus F.
- En chirurgie vétérinaire
- En chirurgie humaine
Absence de consensus dans le traitement des défects calvariens en chirurgie vétérinaire
-
Et si on ne mettait rien ?????
Bibliographie
|