Muffled Heart Sounds in a Dog
- An 11-year-old, 12.5-kg, mixed-breed, male dog presented with a 4-day history of fatigue, abdominal enlargement, and anorexia. The dog became acutely lethargic a few hours before presentation. Clinical examination confirmed lethargy and revealed tachycardia (220 bpm), tachypnea (25 breaths/min), muffled heart sounds, a weak peripheral pulse, jugular distention, a capillary refill time of >2 sec, and ascites.
Auteurs : Drs. C. Bille, E. Bomassi et S. Libermann 06-2010
Centre Hospitalier Vétérinaire des Cordeliers, 29-35 avenue du Maréchal Joffre, 77100 Meaux.
E-mail : cbille@chvcordeliers.com
Cet article a été publié dans : Vetlearn.com | June 2010 | E1- E3
Compendium: Continuing Education for Veterinarians® – ©Copyright 2010 MediMedia Animal Health
Muffled Heart Sounds in a Dog
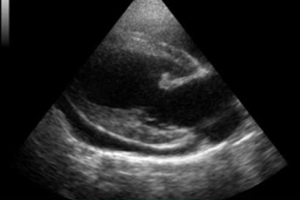
Echocardiography was used to obtain figures A and B.
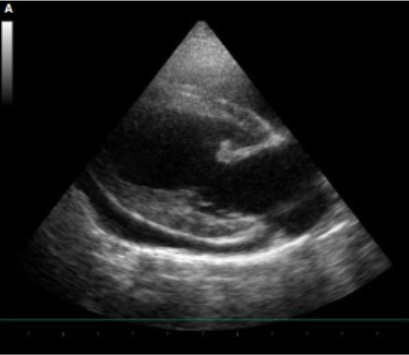
Figure A – Right long-axis view.
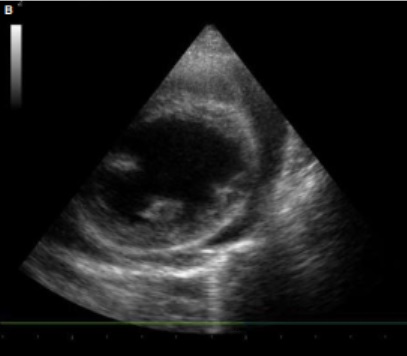
Figure B – Right short-axis view.
Answers and Explanations
- What is the likely explanation for the muffled heart sounds in this patient?
- What underlying etiologies should be considered?
- What further diagnostics should be recommended?
1. Several possible causes of muffled heart sounds exist. An abdominal or thoracic mass that compromises venous return can induce effusion in the abdominal and thoracic cavities. A pericardial, aortic, or cardiac tumor can bleed into the pericardium, impairing right ventricular filling.
Systemic inflammatory response syndrome (SIRS) can induce capillary leakage and effusion into multiple cavities. A coagulation disorder can induce bleeding into multiple (pleural, pericardial, and abdominal) cavities.
The presence of displaced organs in the thoracic cavity (diaphragmatic hernia) should also be investigated.
In this case, echocardiography showed a pericardial effusion and tamponade (Figures C and D). Pericardiocentesis was used to remove 100 mL of serosanguineous fluid. The abdominal fluid was translucent.
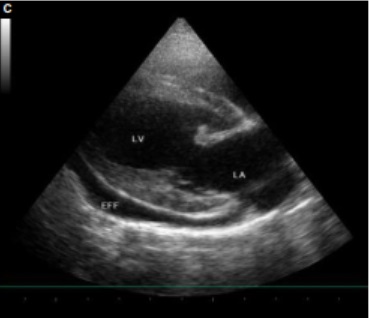
Figure C – Right-long axis view. LA = left atrium, LV = left ventricle, EFF = pericardial effusion
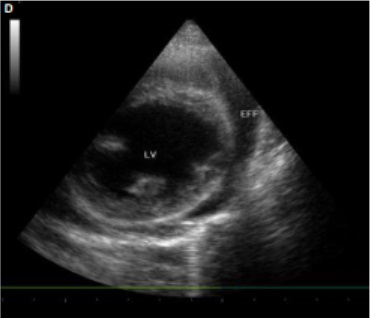
Figure D – Right short-axis view. LV = left ventricle, EFF = pericardial effusion
2. The most common causes of acquired pericardial effusion in dogs are neoplasia and idiopathic causes.1 In one study,2 57% of cases of acquired pericardial effusion were of neoplastic (e.g., hemangiosarcoma, chemodectoma, mesothelioma) origin, 19% were of idiopathic origin, 14% were related to a primary cardiac disease, and 10% were related to another cause (e.g., trauma, infection, SIRS).
The most frequently affected breeds are golden retriever, German shepherd, Saint Bernard, mixed breed, and Labrador retriever.2–4
German shepherds and golden retrievers are predisposed to right atrial hemangiosarcoma.1,2
A predisposition to idiopathic pericardial effusion has been described in German shepherds, Saint Bernards, golden retrievers, and Great Danes.1,2,5
3. Identifying the underlying cause of a pericardial effusion can be challenging. Echocardiography is considered to be the most sensitive and specific noninvasive test; however, every test, including echocardiography, can generate false-positive and false-negative results. In two studies,2,3 a cardiac mass was identified in 37.5% and 29% of dogs presenting with a pericardial effusion.
These results are in accordance with another report,4 which showed that ultrasonography failed to identify 33% of cardiac tumors.
In a group of 14 dogs presented with pericardial effusion, a mass lesion was suspected in one of the six dogs (16.6%) in which a mesothelioma was finally identified and in two of the eight dogs (25%) in which an idiopathic pericardial effusion was finally diagnosed.5
In this case, no mass was visible on echocardiography.
Cytologic evaluation of the pericardial fluid may be helpful but also has its diagnostic limits.
In a study of 19 neoplastic effusions and 31 nonneoplastic effusions, 74% of the neoplastic effusions could not be confirmed by cytologic evaluation and 13% of the nonneoplastic effusions were reported as suspicious for neoplasia.6
This is in accordance with a report5 in which five dogs with mesothelioma and five dogs with idiopathic pericardial effusion were evaluated by cytologic examination of pericardial fluid. Neoplasia was suspected in only 40% of the dogs with mesothelioma. Reactive mesothelial cells were identified in 100% of the mesothelioma samples and in 60% of the idiopathic pericardial effusion samples, making differentiation between etiologies difficult.
In another report,7 cytologic evaluation of pericardial fluid failed to rule out neoplasia in eight of nine dogs (89%) that presented with pericardial effusion. Cytologic evaluation of pericardial fluid from the dog in this case revealed activated mesothelial cells. This finding was suggestive of a mesothelioma.
Histologic examination of pericardial biopsy samples may not offer a definitive diagnosis either.
In one study,5 histologic evaluation identified only 67% of mesotheliomas and 86% of idiopathic pericardial effusions. The remaining mesotheliomas (33%) were still classified as idiopathic.
Histologic evaluation of biopsy samples from the dog in this case found neoplastic cells compatible with a mesothelioma.
* * *
Pericardial mesothelioma usually has a progressive clinical course, and pleural effusion often develops within several weeks or months of pericardectomy.
Discrepancies exist between reported survival times. In a study including eight dogs with pericardial mesothelioma,5 median survival time after biopsy was 60 days (mean: 102 days, range: 15 to 300 days). This is in accordance with other reports.8 On the other hand, one team9 found that dogs with pericardial mesothelioma had a mean survival time of 13.6 months after pericardiectomy was performed.
Another author has described a case in which the patient survived for more than 18 months.10
Because of deteriorating health status, the dog in this case was euthanized at the owner’s request 3 months after diagnosis.
References
|