Patent Ductus Arteriorus in a Family of Chihuahua
Summary
- This report describes a patent ductus arteriosus (PDA) in four puppies from the same family of Chihuahuas, bred from the same mother and from two different litters.
Auteurs : Drs. E. Bomassi, S. Libermann, C. Bille et E. Rattez April 2011 Centre Hospitalier Vétérinaire des Cordeliers, 29 avenue du Maréchal Joffre, 77100 Meaux. E-mail : ebomassi@chvcordeliers.com Cet article a été publié dans : Journal of Small Animal Practice • Vol 52 • April 2011 • © 2011 British Small Animal Veterinary Association : p 213-219
Patent Ductus Arteriorus in a Family of Chihuahua
Summary
- This report describes a patent ductus arteriosus (PDA) in four puppies from the same family of Chihuahuas, bred from the same mother and from two different litters.
- Identification of this congenital anomaly relies on clinical examination, radiography and ultrasonography.
- Three of these puppies were female, and had a type-1 PDA. A conventional surgical ligation was performed on one of them, whilst the others underwent no treatment.
Introduction
A patent ductus arteriosus (PDA) is characterised by the persistence of the fetal blood vessel linking the aorta to the pulmonary trunk. This vessel allows the shunting of blood from the pulmonary circulation towards the general circulation, thus bypassing the fetal lungs, which have yet to be oxygenated. Normally, it seals up during the first few days after birth (Buchanan 1999, 2001). One of the developmental abnormalities of the walls of this vessel (Buchanan and Patterson 2003) is the failure to close off properly, thus creating an abnormal communication (shunt) between the circulation of the left and right sides. In the majority of cases, because of the pressure differential between the aorta and the pulmonary trunk, the shunt flow is from left-to-right. The shunt can sometimes be in the reverse direction, i.e. right-to-left, e.g. in the case of pulmonary arterial hypertension (Buchanan 1999, 2001). The cardiac anatomical and haemodynamic consequences of a persistent arterial duct can lead to the development of cardiac failure (Buchanan 1999, 2001). Treatment of PDA is by conventional surgery using a ligature or a vascular clip or by minimally invasive surgery by intravascular occlusion (Corti and others 2000, Glaus and others 2002, Van Israël and others 2003, Hogan and others 2004, Campbell and others 2006, Goodrich and others 2007, Smith and Martin 2007, Tanaka and others 2007, Achen and others 2008).
This article describes the occurrence of this cardiopathy in a family of Chihuahuas.
Case histories
A three-year-old breeding Chihuahua bitch (F) had two litters 6 months apart, sired by two different males, both Chihuahuas. The first litter (L1), sired by the first, five-year-old male (M1) comprised three puppies, one male (m1) and two females (f1 and f2). The second litter (L2), sired by the second, 18-month-old male (M2) also comprised three puppies, one male (m2) and two females (f3 and f4).
Of the six puppies from these two litters, four puppies (f1, f2, m2 and f3) displayed a PDA.
Examination of the affected puppies
Puppies F1 and F3
Puppy f1 was examined at 7 months of age and puppy f3 at 3 months of age.
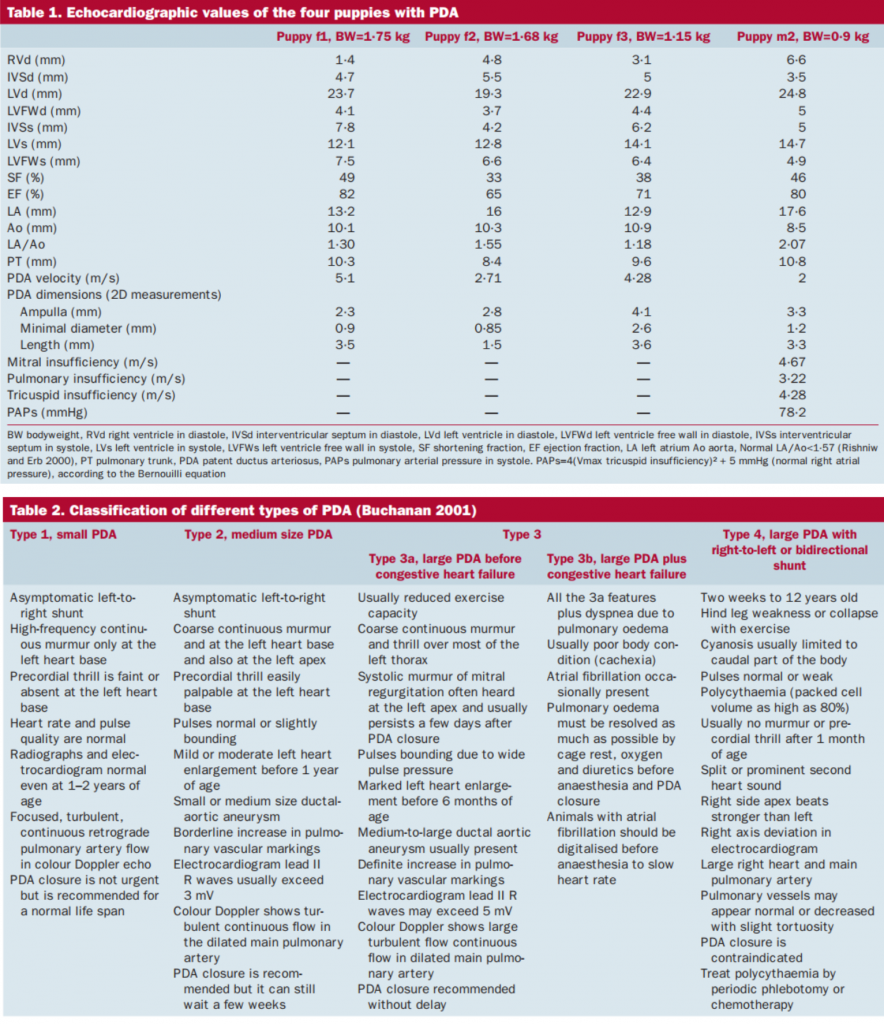
Both these females had unremarkable clinical histories. Their bodyweight was within the normal range for their age and breed. Thoracic auscultation revealed, in both animals, a grade 4/6 left base continuous heart murmur. Echocardiography showed a PDA (Fig 1A and B, Table 1). In both cases, this was a type 1 PDA (Table 2). In accordance with the owners’ wishes, no treatment was given.
Puppy f2
Puppy f2 was examined at 5 months of age with no remarkable clinical history and showing no clinical signs. Her weight was normal. She had a grade 5/6 left base continuous heart murmur. Echocardiography revealed a PDA (Table 1). At the time of examination, there was no other significant anatomical cardiac anomaly detectable by echocardiography, and the size of each chamber was normal (Table 1). This was a type 1 PDA (Table 2).
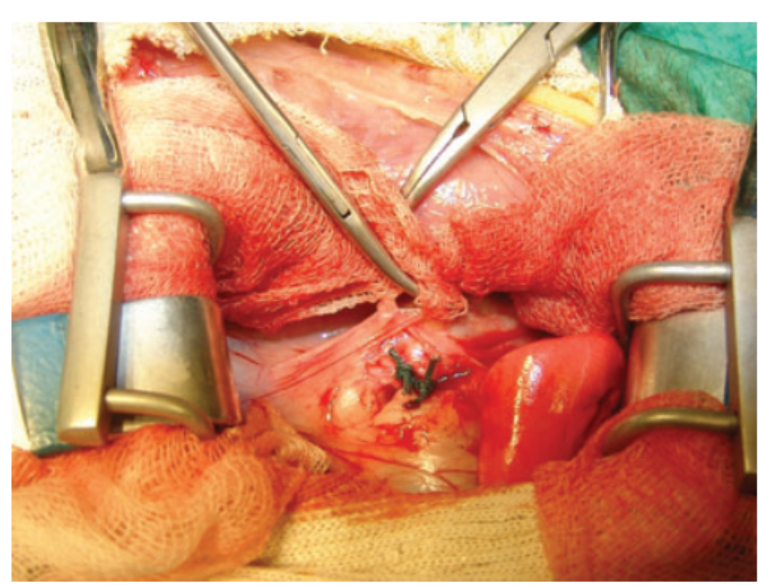
Conventional surgical treatment was elected. After a left-sided intercostal thoracotomy, the vessel was isolated by dissection and ligated (Fig 2). The occlusion was complete, with no residual flow visible on postoperative ultrasonography.
A follow-up examination of the patient at 1 month was unremarkable.
Puppy m2
Puppy m2 was examined at 3 months of age. He showed obviously stunted growth and was very thin (Fig 3A). The mucous membranes were cyanotic (Fig 3B). There was a restrictive dyspnoea. A grade 5/6 systolic murmur was audible; this murmur was principally apical and predominantly left sided. Because of the intensity of the murmur, no other abnormal sounds could be heard (such as split or prominent second heart sound). Thoracic radiographs revealed a significant global cardiomegaly (vertebral heart scale = 14, normal = 9·7 ±0·5; Buchanan and Bucheler 1995), dilatation of the pulmonary trunk, arteries and veins, and an interstitial lung pattern (Fig 4). Echocardiography revealed a dilatation of all four cardiac chambers and the pulmonary trunk, concentric ventricular hypertrophy (Fig 5A and B, Table 1) and a PDA (Table 1). Mitral valve insufficiency, and a high-velocity tricuspid insufficiency, indicative of marked arterial hypertension (systolic pulmonary arterial pressure = 78·2 mmHg), was present. Morphology and kinetics of the mitral valve were normal. The flow in the PDA was reversed, into a right-to-left direction, very probably due to pulmonary hypertension (Stepien 2009). It was considered a type 4 PDA (Table 2).
Faced with such severe clinical signs and a very poor prognosis, euthanasia was advised. A postmortem examination allowed the ductus arteriosus to be dissected out and the dilated vascular structures, and in particular, the pulmonary trunk, to be examined (Fig 6). This macroscopic examination confirmed the findings of the ultrasound examination. On histopathological examination, the ductus arteriosus showed a very thin vessel lining, with a predominance of thick elastic fibres in contact with the aorta. There were very few smooth muscle fibres at this level (Fig 7).
These histological anomalies were identical to those described previously (Buchanan and Patterson 2003).
Examination of non-affected puppies
Puppies m1 and f4 showed neither clinical abnormalities nor any abnormalities on auscultation. No complementary examinations were carried out, as the puppies were not considered affected.
Examination of the bitch F
The bitch F showed no particular clinical signs, and the clinical history was unremarkable. Echocardiography was carried out and no abnormality was detected (Table 3). Specifically, there was no evidence of PDA or other congenital abnormality.
Examination of M1 and M2
The male M1 was normal both clinically and on echocardiography (Table 3). The male M2 had a moderate mitral valve insufficiency of raised velocity (Vmax=6·4 m/s; Table 3). The morphology of the valvular cusps appeared normal, as did the diastolic transmitral flow. In view of the degree of mitral insufficiency and the young age of the dog, this latter was very probably congenital.
Systemic blood pressure (SBP) was measured and was found to be normal (SBP=136 mmHg). This normal pressure measurement rules out systemic hypertension as an explanation of the high value velocity of the mitral regurgitation. The size of the left atrium was mildly increased, with a ratio LA:Ao=1·65 (normal<1·57; Rishniw and Erb 2000).
The two males M1 and M2 and the female F were not related in any way.
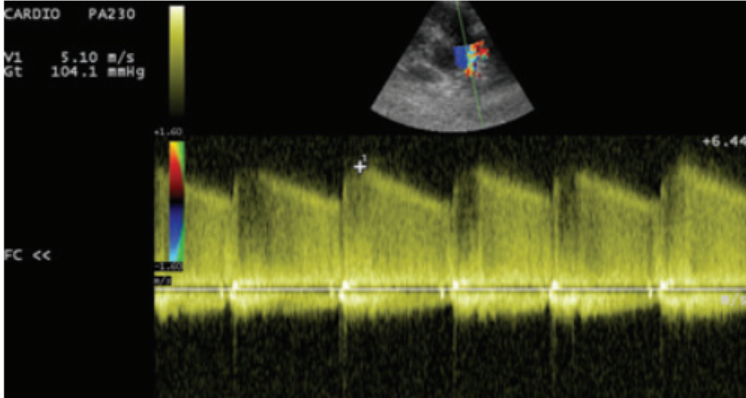
Figure 1 A
PDA of puppies f1 and f3: (A) continuous systodiastolic flow through the patent duct recorded in continuous Doppler mode, left parasternal transaortic view at the heart base of puppy f1 and (B) measurement of the dimensions of the PDA in puppy f3, in 2D mode, left parasternal transaortic view at the heart base. Measurement of the ampulla (D1), the minimum diameter (D2) and its length (D3)
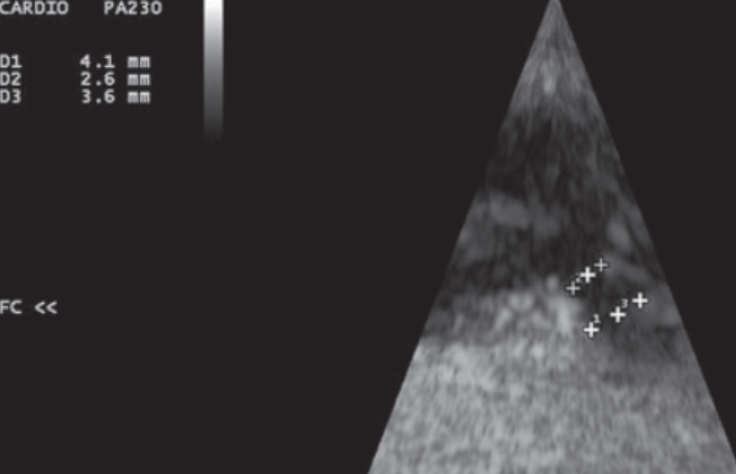
Figure 1 B
Tables 1 et 2

Figure 2
Conventional surgical ligation of the PDA of puppy f2. Double ligature in place

Figure 3 A
Physical appearance of puppy m2: (A) poor general condition, stunted growth and visibly very thin and (B) colour of the mucous membranes of the same puppy: cyanosis

Figure 3 B
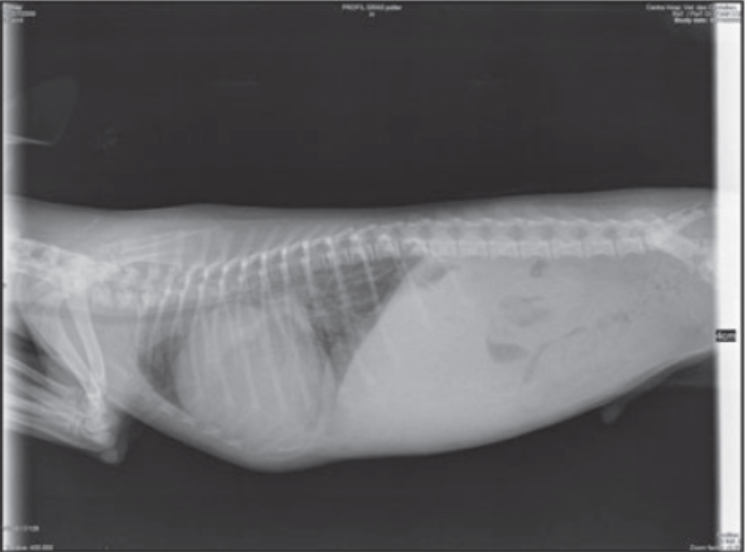
Figure 4
Thoracic radiographs of puppy m2.
Right lateral view: global cardiomegaly, increase in diameter of artery and vein revealing evidence of increased pulmonary blood flow, interstitial pulmonary pattern
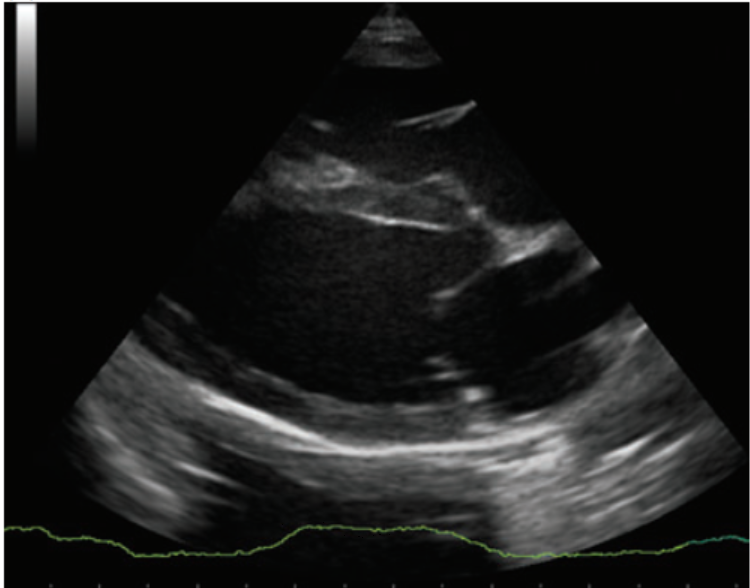
Figure 5 A
Echocardiography of puppy m2: (A) 2D right parasternal long-axis view, dilatation of all four cardiac chambers and ventricular concentric hypertrophy and (B) 2D right parasternal trans-aortic short-axis view. Dilatation of the pulmonary trunk
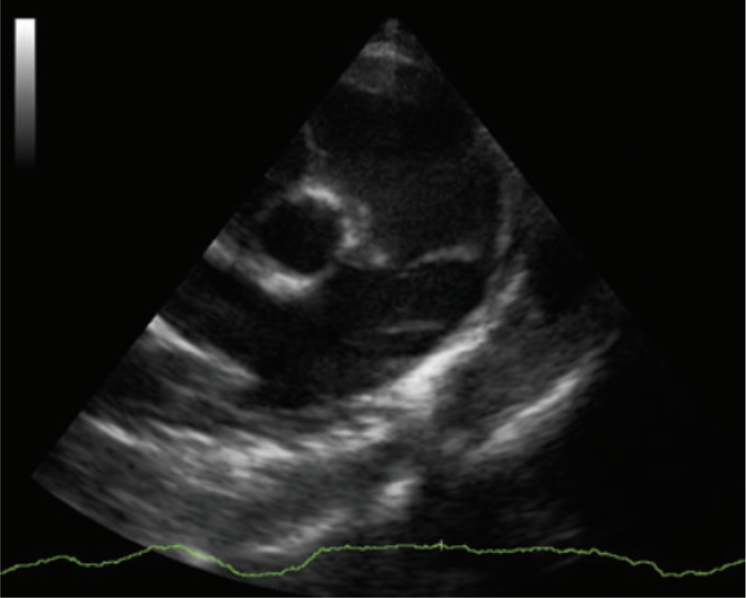
Figure 5 B
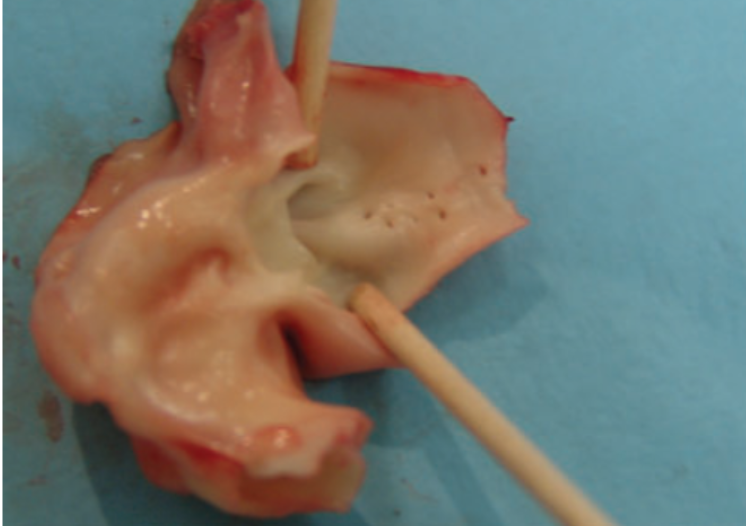
Figure 6
Post-mortem examination views of PDA in puppy m2. Longitudinal dissection of the vessel: conical aspect of the communication between the aorta and the pulmonary trunk. Significant dilatation of the pulmonary trunk
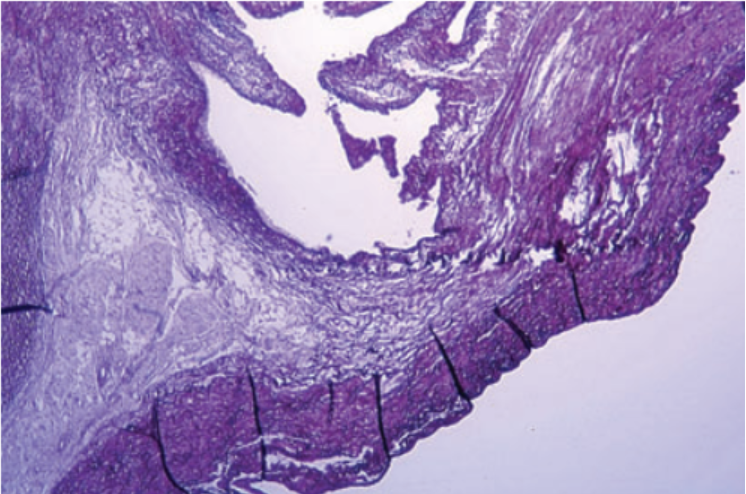
Figure 7
Histopathology of the vessel wall of puppy m2. Multiple very large elastic fibres at contact level of the aorta. Brownish-red stain ×25
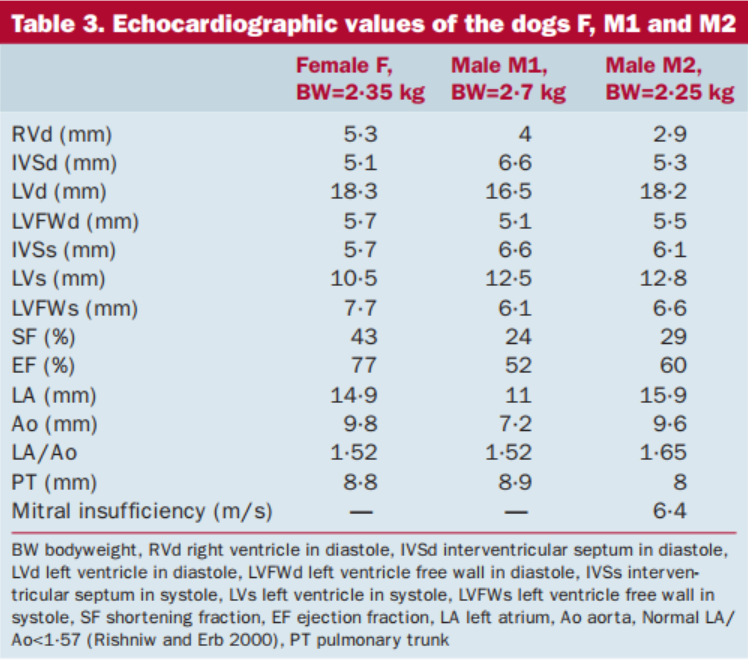
Table 3
Discussion
PDA is a common congenital cardiopathy in the dog. Certain breeds also appear to be predisposed (Buchanan 1999, Van Israël and others 2002). In the poodle, this anomaly is hereditary and the condition is polygenic (Patterson and others 1971). It is probable that the same hereditary basis exists in other cited breeds (Buchanan and Patterson 2003). Females are three times more likely to be affected than males (Van Israël and others 2002).
To the authors’ knowledge, despite being previously reported in the Chihuahua (Buchanan 1999), this is the first description of this congenital cardiopathy in a family of this breed and in a significant number of first-generation individuals.
The study on this family leaves little doubt about the hereditary nature of this anomaly. In accordance with previous descriptions (Buchanan 2001, Van Israël and others 2002), females are more frequently affected than males in this family. Although the mechanics of transmission do not appear clear, female F appears to be involved. A spontaneous genetic mutation in this female is possible and could explain the incidence of PDA in her offspring. With regard to litter L2, the male M2 had a significant mitral insufficiency. Even though this was apparently congenital, it has not been linked with PDA. It is therefore not very likely that there is a link with the PDA of the puppies f3 and m2. Moreover, if there was a link, this would not explain the PDA of the puppies f1 and f2, as the male m1 of the litter L1 was normal, and the males M1 and M2 had no familial links.
The case of puppy m2 needs further explanations. It appears likely that this puppy was initially presented with a large left-to-right shunt. Then left ventricular end diastolic pressure, left atrial pressure and pulmonary venous pressure increased and led to dilatation of left cardiac chambers (Fig 5, dilatation of the left ventricle and left atrium) and congestive heart failure (interstitial lung pattern and overcirculation pattern of the pulmonary vasculature). The poor peripheral perfusion secondary to this congestive heart failure can explain the cyanotic mucous membranes (although no blood gas analysis or pulse oximetry was assessed).
Secondary to the chronic volume overload, pulmonary hypertension may have developed and led to a right-to-left shunt. However, no histopathological examination was performed on the lungs from dog m2, and so the presence of a primary pulmonary hypertension due to primary vascular lesions could not be evaluated and not definitively ruled out.
Finally, in a reversed shunt, the murmur is usually very faint or inaudible. In this case, the murmur was due to mitral and tricuspid regurgitation. Mitral regurgitation appeared to be a functional sequela to annular dilatation without abnormalities of the mitral valve. Tricuspid regurgitation may well be secondary topulmonary hypertension.
The aetiology of PDA is uncertain but would appear to correspond macroscopically to an anomaly of the size of the vessel and histologically to an abnormal distribution of different types of fibres. Smooth muscle fibres, which enable the tightening and occlusion of the vessel, are comparatively sparsely represented, with respect to elastic fibres, in contact with the aorta (Buchanan and Patterson 2003).
The histopathological examination carried out on the PDA of puppy m2 confirmed the same anomalies as those described above and support these observations (Fig 7).
Clinical findings in the puppies that had a PDA were typical. According to the literature, in 90% of cases, a persistent continuous murmur is audible, and is often an incidental finding (Van Israël and others 2002). Other clinical signs (stunted growth, cough and dyspnoea) are not consistently seen and appear at a later stage. The average age of presentation of asymptomatic animals is 7 months, compared with 24 months for those presented with clinical signs (Van Israël and others 2002). In the family reported in this article, the animals examined were still very young and did not yet show any generalised clinical signs (females f1, f2 and f3). Only the puppy m2, with a reverse flowPDA, showed overt clinical signs, despite its young age, which necessitated euthanasia.
Ultrasonography is the complementary examination of choice in identifying a PDA and evaluating the haemodynamic and anatomic consequences.
On echocardiography, demonstration of continuous systodiastolic turbulence in the pulmonary trunk is very suggestive of PDA. The duct can be visualised in 96% of affected animals by the left parasternal approach, taking a basal short-axis view, either in two-dimensional (2D) mode, as in all the cases in this report or in Doppler colour mode (Saunders and others 2007, Schneider and others 2007). The 2D mode is the more precise of these two modes for assessing a PDA (Schneider and others 2007).
The treatment for PDA is surgical. The occlusion of the vessel can be carried out by a conventional ligature technique, as in the case of puppy f2, or by the use of vascular clips, spring coil embolisation or a canine amplatz® prosthesis via a percutaneous catheter (Corti and others 2000, Glaus and others 2002, Van Israël and others 2003, Hogan and others 2004, Campbell and others 2006, Goodrich and others 2007, Smith and Martin 2007, Tanaka and others 2007, Achen and others 2008). The perioperative mortality rate is between 2·5 and 5·6%, whichever the technique chosen. Complete closure of the vessel with a single operation is obtained in 57 to 94% of surgical cases. Survival rates in dogs treated surgically are 92% at 1 year and 87% at 2 years (Bureau and others 2005). In the absence of surgical intervention, only 36% of the animals survive the first year (Stanley and others 2003). As regards the two puppies not treated, f1 and f3, follow-ups will be of interest in evaluating the occurrence of complications linked to PDA, and in particular, cardiac failure.
Conslusion
This article is possibly the first description of PDA in a family of Chihuahuas. The characteristics of the anomaly in this family group are identical to those formerly described in other breeds (clinical presentation, ultrasonography and histopathology). The hereditary nature in this family appears clear, even though the mode of transmission has not been fully identified. It may be that subsequent observations in this breed will shed further light on this congenital abnormality.
Acknowledgment
The authors thank Dr Agnes Poujade, LAPVSO Laboratory, Toulouse, France, and Oniris Veterinary School, France, for histopathological analysis. Dr Doran Ivan, MRCVS, Oniris Veterinary School, France, for reviewing this article.
Conflict of interest
None of the authors of this article has a financial or personal relationship with other people or organisations that could inappropriately influence or bias the content of the paper.
References[1] ACHEN, S. E., MILLER. M. W., GORDON, S. G. SAUNDERS, A. B., ROLLAND, R. M. & DROURR, L. T. (2008) Transarterial ductal occlusion with the Amplatzer vascular plug in 31 dogs. Journal of Veterinary Internal Medicine 22, 1348-1352 [2] BUCHANAN, J. W. (1999) Prevalence of cardiovascular disorders. In: Canine and Feline Cardiology. 2nd edn. Eds P. Fox, D. Sisson and N. S. Moïse. W. B. Saunders Co., Philadelphia, PA, USA. pp 457-470 [3] BUCHANAN, J. W. (2001) Patent ductus arteriosus. Morphology, pathogenesis, types and treatment. Journal of Veterinary Cardiology 3, 7-16 [4] BUCHANAN, J. W. & BUCHELER, J. (1995) Vertebral scale system to measure canine heart size in radiographs. Journal of American Veterinary Medical Association 206, 194-199 [5] BUCHANAN, J. W. & PATTERSON, D. F. (2003) Etiology of patent ductus arteriosus in dogs. Journal of Veterinary Internal Medicine 17, 167-171 [6] BUREAU, S., MONNET, E. & ORTON, E. C. (2005) Evaluation of survival rate and prognostic indicators for surgical treatment of left-to-right patent ductus arterio-sus in dogs: 52 cases (1995-2003). Journal of American Veterinary Medical Association 227, 1794-1799 [7] CAMPBELL, F. E., THOMAS, W. P., MILLER, S. J., BERGER, D. & KITTLESON, M. D. (2006) Immediate and late outcomes of transarterial coil occlusion of patent ductus arteriosus in dogs. Journal of Veterinary Internal Medicine 20, 83-96 [8] CORTI, L. B., MERKLEY, D., NELSON, O. L. & WARE, W. A. (2000) Retrospective evaluation of occlusion of patent ductus arteriosus with hemoclips in 20 dogs. Journal of American Animal Hospital Association 36, 548-555 [9] GLAUS, T. M., BERGER, F., AMMANN, F. W., KLOWSKI, W., OHLERT, S., BOLLER, M., KÄSTNER, S., REUSCH, C. E. & SISSON, D (2002) Closure of large patent ductus arteriosus with a self-expanding duct occluder in two dogs. Journal of Small Animal Practice 43, 547-550 [10] GOODRICH, K. R., KYLES, A. E., KASS, P. H. & CAMPBELL, F. (2007) Retrospective comparison of surgical ligation and transarterial catheter occlusion for treatment of patent ductus arteriosus in two hundred and four dogs (1993-2003). Veterinary Surgery 36, 43-49 [11] HOGAN, D. F., GREEN, H. W., GORDON, S. & MILLER, M. W. (2004) Transarterial coil embolization of patent ductus arteriosus in small dogs with 0.025-inch vascular occlusion coils: 10 cases. Journal of Veterinary Internal Medicine 18,325-329 [12] PATTERSON, D. F., PYLE, R. L., BUCHANAN, J. W., TRAUTVETTER, E. & ABT, D. A. (1971) Hereditary patent ductus arteriosus and its sequelae in the dog. Circulation Research 29, 1-13 [13] RISHNIW, M. & ERB, H. N. (2000) Evaluation of four 2-dimensional echocardiographic methods of assessing left atrial size in dogs. Journal of Veterinary Internal Medicine 14, 429-435 [14] SAUNDERS, A. B., MILLER, M. W., GORDON, S. G. & BAHR, A. B. (2007) Echocardiographic and angiographic comparison of ductal dimensions in dogs with patent ductus arteriosus. Journal of Veterinary Internal Medicine 21, 68-75 [15] SCHNEIDER, M., HILDEBRANDT, N., SCHWEIGL, T. & WEHNER, M. (2007) Transthoracic echocardiographic measurement of patent ductus arteriosus in dogs. Journal of Veterinary Internal Medicine 21, 251-257 [16] SMITH, P. J. & MARTIN, M. W. (2007) Transcatheter embolisation of patent ductus arteriosus using an Amplatzer vascular plug in six dogs. Journal of Small Animal Practice 48, 80-86. [17] STANLEY, B. J., LUIS-FUENTES, V. & DARKE, P. G. (2003) Comparison of the incidence of residual shunting between two surgical techniques used for ligation of patent ductus arteriosus in the dog. Veterinary Surgery 32, 231-237 [18] STEPIEN, R. L. (2009) Pulmonary arterial hypertension secondary to chronic left-sided cardiac dysfunction in dogs. Journal of Small Animal Practice 50, 34-43 [19] TANAKA, R., SODA, A., SAIDA, Y., SUGIHARA, K., TAKASHIMA, K., SHIBAZAKI, A. & YAMANE, Y. (2007) Evaluation of the efficacy and safety of coil occlusion for patent ductus arteriosus in dogs. Journal of Veterinary Medical Science 69, 857-859 [20] VAN ISRAËL, N., DUKES-MCEWAN, J. & FRENCH, A. T. (2003) Long-term follow-up of dogs with patent ductus arteriosus. Journal of Small Animal Practice 44, 480-490 [21] VAN ISRAËL, N., FRENCH, A. T., DUKES-MCEWAN, J. & CORCORAN, B. M. (2002) Review of left-to-right shunting patent ductus arteriosus and short term outcome in 98 dogs. Journal of Small Animal Practice 43, 395-400 |