
Risk of anaesthetic mortality in dogs and cats
Objective
- To evaluate the anaesthetic death risk for dogs and cats in a French private practice.
Auteurs : Drs. C. Bille*, V. Auvigne°, S. Libermann*, É. Bomassi*, P. Durieux* et É. Rattez* 12-12-2011
*Centre Hospitalier Vétérinaire des Cordeliers, 29-35 avenue du Maréchal Joffre, 77100 Meaux.
°Ekipaj, Angers, France
E-mail : cbille@chvcordeliers.com
Cet article a été publié dans : Veterinary Anaesthesia and Analgesia, 2012, 39, 59–68
Risk of anaesthetic mortality in dogs and cats:
an observational cohort study of 3546 cases
Abstract
Objective
To evaluate the anaesthetic death risk for dogs and cats in a French private practice.
Study design
Observational cohort study.
Animal population
All small animals anesthetized at the Centre Hospitalier Vétérinaire des Cordeliers between April 15th, 2008 and April 15th, 2010.
Methods
General anaesthesia was defined as a drug-induced unconsciousness characterised by a controlled and reversible depression of the central nervous system and analgesia, sufficient to allow endotracheal intubation. Patient outcome (alive or dead) was assessed at the end of anaesthesia defined as the meeting point of the return of consciousness, rectal temperature >36 C and ability to maintain sternal recumbency. Death occurring during anaesthesia was recorded. Relationship between anaesthetic death and ASA status, species, age, nature of the procedure, anaesthetic protocol and occurrence of epidural administration of a combination of morphine and bupivacaine were analysed.
Results
During the study period 3546 animals underwent general anaesthesia. The overall death rate in the present study was 1.35% (48 in 3546, 95% CI 0.96–1.75). The death rate of healthy animals (ASA 1 and 2) was 0.12% (3 in 2602 95% CI 0.02–0.34). For sick animals (ASA status 3 and over), the overall death rate was 4.77% (45 in 944 95% CI 3.36–6.18). The death rates in the ASA 3, 4 and 5 categories were 2.90%, 7.58% and 17.33%, respectively. The main factor associated with increased odds of anaesthetic death in ASA categories 3 and over was poor health status (ASA physical status classification). The nature of the procedure the patient underwent and epidural administration of a combination of morphine and bupivacaine were not correlated with the occurrence of death during anaesthesia. Neither species nor age effects were detected.
Conclusion and clinical relevance
Specific factors were associated with increased odds of anaesthetic death, especially poor health status. Efforts must be directed towards thorough preoperative patient evaluation and improvement of clinical conditions if possible. Identification of risk factors before anaesthesia should lead to increased surveillance by trained staff. This could result in better outcomes.
Introduction
In the last 30 years, the risk of anaesthetic death has been studied in dogs and cats by teams in different countries (Clarke & Hall 1990; Dodman & Lamb 1992; Dyson et al. 1998; Hosgood & Scholl 1998, 2002; Gaynor et al. 1999; Joubert 2000; Nicholson & Watson 2001; Williams et al. 2002; Redondo et al. 2007; Brodbelt et al. 2006, 2008a,b; Alef et al. 2008).
The most recent study of anaesthetic deaths (Brodbelt et al. 2008a) included 98,036 dogs and 79,178 cats and defined anaesthetic or sedationrelated death as a perioperative death (including euthanasia) occurring after pre-medication and within 48 hours of termination of the procedure, except when death or euthanasia was due solely to inoperable surgical or pre-existing medical conditions. Considering animals of all American Society of Anesthesiologists (ASA) grades, cumulative incidences of anaesthetic and sedation-related death were reported to be 0.17% in dogs and 0.24% in cats. This is higher than the 0.01–0.02% reported in human anaesthesia (Biboulet et al. 2001; Newland et al. 2002).
There is no consensus on the definition of anaesthetic mortality (Arbous et al. 2001). Discrepancies between different reports may result from the studied population. Some authors have included animals that underwent general anaesthesia while others included patients undergoing either general anaesthesia or sedation. Variations may be seen regarding the cause of death, some authors including death of any origin whilst others only considering death that cannot be explained by pre-existing medical conditions or surgical complications.
Variations also occur over the study period. Sometimes, this is not clearly defined. Others define the study period as the time of anaesthesia or the time of surgery or set an end point between a few hours (Williams et al. 2002) to 48 hours after termination of the procedure (Brodbelt et al. 2006, 2008a,b).
In small animal practice, the risk of death during anaesthesia has shown to be related to different factors. It was increased in cats compared to dogs (Brodbelt et al. 2008a), in some particular breeds (Clarke & Hall 1990; Brodbelt et al. 2008a), in patients older than 12 years (Hosgood & Scholl 1998; Brodbelt et al. 2006, 2008b), in patients weighing <5 kg (Brodbelt et al. 2008b), in patients with poor health status (Clarke & Hall 1990; Dyson et al. 1998; Hosgood & Scholl 1998, 2002; Brodbelt et al. 2006, 2008a,b), if anaesthesia took place in a referral centre (Gaynor et al. 1999; Brodbelt et al. 2006, 2008a), if a procedure was urgent (Brodbelt et al. 2008b), if a surgical procedure was considered as major (Brodbelt et al. 2008b), if specific agents were used (Dyson et al. 1998) and if an inhalant agent alone was used for induction (Brodbelt et al. 2008b).

Figure 1 – Flow diagram of the recruitment and follow-up of the anaesthetic cases.
The aim of this study was to evaluate the anaesthetic death risk for dogs and cats in a French private practice. The authors hypothesised that cats would be at greater risk than dogs and that the anaesthetic death risk would be related to the patient’s health status and age but not the nature of the drug used for induction of anaesthesia. To the author’s knowledge, this is the first cohort study of small animal anaesthetic deaths undertaken in a single private practice in France.
Methods
We used an observational cohort study design. The observational character of the data collection implies that any decision made by an attending veterinarian on the anaesthetic procedure was not influenced in any way by the study design.
Patients’ recruitment
This cohort study recruited all dogs and cats that underwent general anaesthesia at the Centre Hospitalier Vétérinaire des Cordeliers between April 15th 2008 and April 15th 2010 (Fig. 1). General anaesthesia was defined as a drug-induced unconsciousness characterised by a controlled and reversible depression of the central nervous system (CNS) and analgesia, sufficient to allow endotracheal intubation (Thurmon & Short 2007). Patients that were sedated or anaesthetized in order to be euthanased were not included. Sedation was defined as chemical restraint insufficient to allow endotracheal intubation.
The study period commenced when general anaesthesia was induced by administration of an injectable agent, whatever the route (intravenous (IV) or intramuscular (IM)), or with isoflurane and ended with the end of anaesthesia. This end was set at the last point at which anaesthetized patients could be systematically checked in a comparable manner. It was therefore defined as the meeting point of the return of consciousness, rectal temperature >36 C and ability to maintain sternal recumbency.
Animals that were euthanased during anaesthesia because of medical reasons were excluded from the study.
Data collection
For all patients that were included, identification data, species and age were recorded. Prior to anaesthetic induction, on the basis of history and clinical examination, the attending anaesthetist assessed the patient’s ASA status and whether it would need laboratory tests or not. He then decided which of the anaesthetic protocols (see below) would be used. Any potential bias from such a decision was addressed by introducing the ASA status as a covariate in the final model Epidural administration of a combination of morphine and bupivacaine by means of an injection or by placement of an epidural catheter was recorded.
The type of procedure the patient underwent was defined as: examination (chemical restraint was needed to perform a non-invasive procedure), orthopaedic or soft tissue surgery. Death occurring during anaesthesia was recorded.
Anaesthetic regimens
Premedication, induction and maintenance agents were recorded. For the data analysis, all premedication regimens were gathered in a ‘premedication’ category. As a consequence, the nature of the substance used and the route of administration were not taken into account. Any patient that did not receive premedication was included in a ‘No’ ‘premedication’ category.
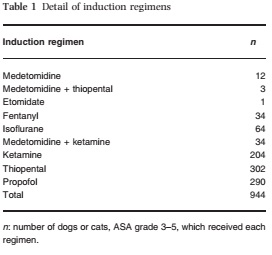
Induction regimens were grouped into four categories: ‘Ketamine’, ‘Thiopental’, ‘Propofol’ and ‘Other induction’. ‘Other induction’ included the use of fentanyl, isoflurane, etomidate, or their association with ketamine or thiopental (Table 1). Dogs given medetomidine or dexmedetomidine such that endotracheal intubation was carried out (n = 12) were also included in this group.
Two groups of maintenance regimes were defined: patients that received isoflurane and patients that did not. Patients that did not receive isoflurane were anaesthetized by means of total IV anaesthesia or IM injection of the induction agent with no further maintenance agent.
The overall anaesthetic regimen was then defined by the combination of the premedication, the induction and the maintenance regimens. Four groups were defined (Table 2):
- Use of premedication, induction of anaesthesia with ketamine, maintenance with isoflurane.
- Use of premedication, induction of anaesthesia with thiopental, maintenance with isoflurane.
- Use of premedication, induction of anaesthesia with propofol, maintenance with isoflurane.
- Use of any other anaesthetic regimen. This represented 66 different regimens.
For statistical means, animals were grouped according to their age. Groups were defined arbitrarily to obtain four categories of equal importance as shown in Table 2.
Data analysis
The data analysis was conducted following a two-step approach. As a first step, bivariate analysis was performed to analyse the relationship between ASA score and mortality (Mann–Whitney/ Wilcoxon Two-Sample Test, EpiInfo 3.5.1; Centers for Disease Control and Prevention, GA, USA). 95% Confidence Intervals were calculated using the normal approximation when n(1 – p) > 4 and the binomial exact method in other cases (Epidat 3.1; Epidat : PanAmerican Health Organization, WA D.C., USA).
As a second step, because of the null to very low mortality in animals of ASA score 1 or 2 (see Results), only animals of ASA score of 3 or more were included. In other words, because the occurrence of the outcome is rare in the subpopulation of ASA score 1 or 2, the analysis of the relationship between death and other variables is of no benefit. In this second step, univariate and bivariate analyses were carried out, followed by a multivariate analysis of the data. The statistical unit was the animal and death the outcome variable.
Logistic regression models were created using the GLM procedure of R software 2.9.0 (R Foundation for Statistical Computing, Austria). ‘ASA category’, ‘Species’, ‘Type of procedure’, ‘Anaesthetic protocol’, ‘Epidural’ and ‘Age’ were set as explanatory variables. The probability of wrongly rejecting the null hypothesis was set to 5%. A backward procedure was used.
Variables were kept in the model if p <0.15. Two-way interactions were tested and kept in the model if p <0.05. For assessing the fit of the models receiver-operating characteristic (ROC) curves were constructed and the areas under curves (AUCs) were calculated.
Results
During the study period, 3546 animals underwent general anaesthesia. Animals lost to follow-up were estimated to be 35. The number of patients euthanased for medical reasons during general anaesthesia was evaluated at <10 (Fig. 1).
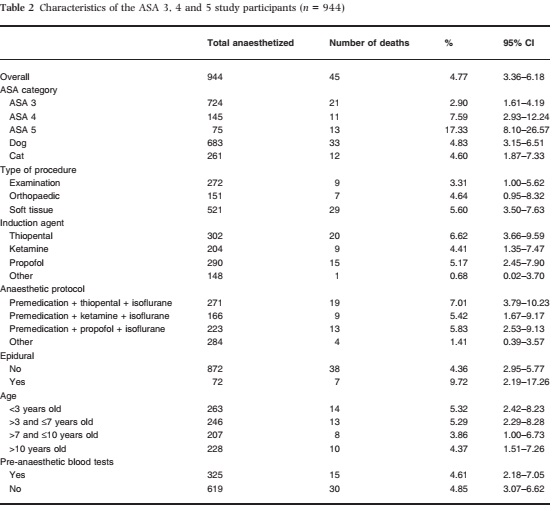
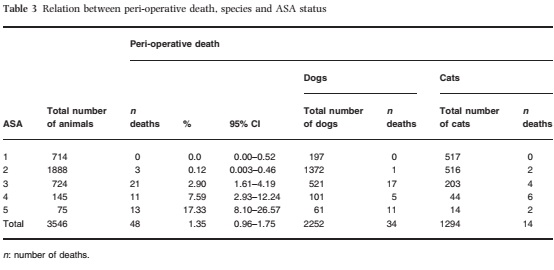
The first-step (univariate) analysis revealed that 48 animals out of 3546 (1.35%, 95% CI 0.96–1.75) died. No animal died in the ASA 1 category. The death rate increased with each grade of ASA status (Table 3). The second-step (multivariate) analysis was performed on the ASA 3, 4 and 5 categories. Nine hundred and forty-four patients of ASA status 3, 4 and 5 were included (Fig. 1). The characteristics of these 944 patients are shown in Table 2.
Forty-five (4.77%, 95% CI 3.36–6.18) died during anaesthesia (Table 2).
When considering the multivariate model (Table 4), increasing ASA status was associated with increased odds of anaesthetic death. Also, when compared to the group ‘other anaesthetic protocol’, the group ‘premedication + thiopental + isoflurane’ was associated with increased odds of anaesthetic death. Increasing ASA category from 3 to 4 was associated with a 3.7-fold increase in the odds of death (p = 0.001, 95% confidence interval (CI) [1.7–8.1]). Increasing ASA category from 3 to 5 was associated with a 13.4-fold increase in the odds of death (p < 0.001, 95% CI [5.8–30.4]).
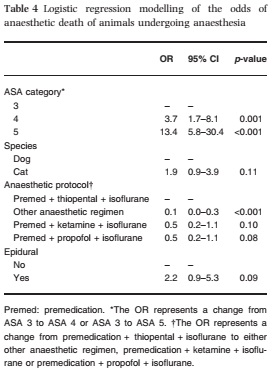
Compared to the group ‘premedication + thiopental + isoflurane’, the group ‘Other anaesthetic protocol’ was associated with a 10-fold decrease in the odds of death (p < 0.001, 95% CI [0.0–0.3]).
Compared to the group ‘premedication + thiopental + isoflurane’, the group ‘premedication + propofol + isoflurane’ showed a tendency for a decrease in the odds of death (p = 0.08, 95% CI [0.2–1.1]).
Compared to the group ‘premedication + thiopental + isoflurane’, the group ‘premedication + ketamine + isoflurane’ showed a tendency for decrease in the odds of death (p = 0.10, 95% CI [0.2–1.1]).
Although not statistically significant, there was a tendency for cats to be more at risk of dying during anaesthesia than dogs (p = 0.11, 95% CI [0.9–3.9]). There was a tendency for animals receiving an epidural combination of morphine and bupivacaine to be more at risk of anaesthetic death (p = 0.09, 95% CI [0.9–5.3]). After adjusting for other variables, the odds of death associated with the type of procedure were not significantly different. No age (data not shown) effect was detected.
None of the interaction terms were significant and were therefore dropped out of the model. The AUC of the model was 0.74 indicating acceptable discrimination properties (Hosmer & Lemeshow 2000).
Discussion
The overall death rate in the present study was 1.35%. Results suggest that ASA status was significantly associated with increasing the odds of anaesthetic death in dogs and cats. When considering patients of ASA status 3 and over, the use of an anaesthetic protocol that included premedication, induction with thiopental and maintenance with isoflurane, was associated with increased odds of anaesthetic death when compared to the group ‘other anaesthetic regimen’. Results also suggest that, although not significant, there is a tendency for cats and animals receiving an epidural injection to be more at risk of anaesthetic death. Age was not found to be associated with an increase in the odds of death.
Many of the previously published studies have reported anaesthetic death rates of between 0.17% and 0.43% (Clarke & Hall 1990; Dodman & Lamb 1992; Dyson et al. 1998; Gaynor et al. 1999; Joubert 2000; Williams et al. 2002; Brodbelt et al. 2006, 2008a; Alef et al. 2008), which are lower than those reported here. However, there are two surveys (Hosgood & Scholl 1998, 2002) which have reported death rates similar to those seen in this current study.
As discussed earlier, it is difficult to compare different studies on anaesthetic death as case definitions and methods differ. It must also be remembered that in the earlier surveys, anaesthetic agents differed, and the computing power to calculate odds ratios was not always available.
This study was designed to provide a high rank of evidence when considering anaesthetic death risk factors. A cohort observational study was thought to be adequate (Holmes 2007). Major difficulties encountered when building this type of cohort observational study were thought to be: 1) including a representative group of the exposed population; and 2) limiting the loss related to poor followup. Therefore it was decided that all anaesthetized patients should be included.
Some animals were lost to follow up when data were not recorded by the administrator. Reasons included the administrator being unaware that anaesthesia had taken place, usually for a minor, short and uneventful procedure. Occasionally the administrator postponed filling out the data sheet and had forgotten a procedure that took place at the end of the day. It was estimated that one animal was lost to poor follow-up every 3 weeks; a total of 35 patients.
The end of the study period was defined as the meeting point of the return of consciousness, rectal temperature >36 C and ability to maintain sternal recumbency. An end point of 48 hours after the procedure as set in veterinary (Brodbelt et al. 2006, 2008a,b) and human literature (Newland et al. 2002) or at the discharge of the patient (Wolters et al. 1996) would probably have increased the death rate, as animals that died in the immediate postoperative period would then have been taken into account. In the current study, from practice,
this type of end point would have led to a selection bias by excluding many animals undergoing minor procedures that were not seen 48 hours after the procedure took place.
The major reason for euthanasia during anaesthesia was the diagnosis of an inoperable tumour. As these animals were to be excluded from the study, no data were prospectively recorded, and therefore, the number of euthanased patients was estimated retrospectively. The authors acknowledge it would have been preferable to record the number of such patients.
The study’s objective was to evaluate anaesthetic death of any cause, so no attempt was made to classify the cause of death. Thus deaths from medical or surgical complications were included.
This is different from other studies (Brodbelt et al. 2006, 2008a,b), where authors defined anaesthetic or sedation-related death as death that could not be explained totally by pre-existing medical or surgical complications.
A potential selection bias comes from the fact that the Centre Hospitalier Vétérinaire des Cordeliers is a referral centre. A difference in anaesthetic mortality has been observed when comparing practice-based studies (Clarke & Hall 1990; Dodman & Lamb 1992; Dyson et al. 1998; Joubert 2000; Williams et al. 2002), referral-studies (Hosgood & Scholl 1998, 2002; Gaynor et al. 1999; Brodbelt et al. 2006) or both (Brodbelt et al. 2008a,b). Referral practices usually anaesthetize a greater proportion of patients classified in the ASA 3, 4 and 5 categories. In our case, these categories represent 26.6% of the anaesthetized population. This is more than the 5–10% described in the practice-based studies (Clarke & Hall 1990; Dyson et al. 1998), and could explain the higher percentage of deaths in our study.
In this study, sick patients, as assessed by ASA score, had higher risk of anaesthetic death than did healthy animals. The ASA status is correlated to anaesthesia-related death in humans (Vancanti et al. 1970; Wolters et al. 1996; Jones & Cossart 1999; Biboulet et al. 2001; Newland et al. 2002) and in domestic animals (Clarke & Hall 1990; Dodman & Lamb 1992; Dyson et al. 1998; Hosgood & Scholl 1998, 2002; Brodbelt et al. 2006, 2008a,b). The death rate increases with each grade of ASA status (Table 3). This suggests that there is a causal relationship between these variables. The published absolute mortality rates of the ASA classes has shown variations in veterinary studies, with 0.05–0.10% for ASA 1 and 2 categories and 1–2% for ASA 3, 4 and 5 categories (Dyson et al. 1998; Hosgood & Scholl 1998, 2002; Brodbelt et al. 2006, 2008a,b). Our data show a mortality rate of 0.12% for ASA 1 and 2 categories and 4.76% for ASA 3, 4 and 5 categories. These variations can be explained in part by differences in assessment of the patient’s ASA physical status. In our case, we tried to limit this variability by having one attending veterinarian (CB) review and, if necessary, reassess the ASA status, on the basis of the patient charts.
The anaesthetic protocol was established by the veterinarian in charge, in light of his experience. Anaesthetist’s experience is a subjective concept and is hard to analyse. It refers to numerous factors as patient condition, species, breed, body weight, nature of the illness, nature of the procedure, personal habits and preferences, personal perception and interpretation of an illness, owners’ wishes, time of the day, work load, experience of co-workers (nurse and/or surgeon), and economic aspects. Many of these factors could not be tested as variables in the logistic regression models and this could have led to a selection bias.
The ‘premedication + thiopental + isoflurane’ group was statistically correlated to anaesthetic deaths when compared to the group ‘other anaesthetic regimen’. Although not statistically significant, there was a tendency for animals in the group ‘premedication + thiopental + isoflurane’ to be more at risk of anaesthetic death when compared to those in groups ‘premedication + propofol + isoflurane’ and ‘premedication + ketamine + isoflurane’. This was unexpected. There is no clear explanation for this finding. The Centre Hosptalier Vétérinaire des Cordeliers tends to use an anaesthetic protocol that includes premedication, an injectable induction agent and maintenance using inhalation anaesthesia with isoflurane in very critical patients, which could lead to a selection bias, as these protocols might therefore include a relatively larger number of anaesthetic deaths. This potential bias was addressed by introducing the ASA status as a covariate in the final model.
The authors have analysed the raw interactions between anaesthetic protocol and variables that were shown to increased the odds of anaesthetic death or to have tendency to increase the odds of anaesthetic death in the logistic regression model (e.g. ASA status, epidural and species). However, anaesthetic protocols were not randomly assigned.
Therefore, when considering raw associations, most variables are significantly associated. Moreover, ASA status and anaesthetic protocol, epidural injection and anaesthetic protocol, species and anaesthetic protocol were significantly correlated (data not shown). Because of these numerous correlations it was decided that raw interactions would not be interpreted and that only the logistic regression model would be satisfactory.
No satisfactory explanation was identified to explain why the ‘premedication + thiopental + isoflurane’ group was overrepresented in anaesthetic deaths. Using an ‘other protocol’ when compared to ‘premedication + thiopental + isoflurane’ was associated with a 10-fold decrease in the odds of anaesthetic death. This finding was expected. It is probable that, despite ASA classification, anaesthetist’s experience leads to a subjective evaluation of the risk. This can lead to the establishment of ‘another protocol’. This leads to a selection bias.
The ‘other protocol’ category may then appear safer when in reality it is not and contains animals that where subjectively judged to be less at risk for anaesthetic death. As other protocol included many variations, numbers within any subcategory were too small for analysis.
The roles of premedication, induction and maintenance drugs in anaesthetic death have been studied (Clarke & Hall 1990; Dyson et al. 1998; Brodbelt et al. 2006, 2007, 2008a,b). The use of either acepromazine, atropine or medetomidine in premedication has been found to decrease the odds of anaesthetic death (Clarke & Hall 1990; Dyson et al. 1998; Brodbelt et al. 2006, 2008a). The use of xylazine in the anaesthetic protocol in dogs has been shown to be associated with an increase in the odds of anaesthetic death (Dyson et al. 1998). No correlation has been found previously between the use of either ketamine, thiopental of propofol and anaesthetic death (Dyson et al. 1998; Brodbelt et al. 2006, 2008a).
Dog owners might be more likely to seek medical attention than cat owners. A selection bias could therefore enhance the association between dogs and anaesthesia-related death, compared to cats. Also, cats’ health status is, in general, less easily assessable than dogs’, possibly resulting in poorer preoperative assessment of the feline patients. Finally, a type-II error could explain the tendency for cats to be more prone to anaesthetic death when compared to dogs. It could be induced by the small number of subjects (944) enrolled in our study. Therefore, the tendency for cats to be more prone to anaesthesia-related death could have been significant if a greater number of patients had been included. In other studies there are conflicting results. Some authors concluded that cats were more prone to anaesthetic death when compared to dogs (Clarke & Hall 1990; Hosgood & Scholl 1998, 2002; Brodbelt et al. 2008a). Other teams found no correlation (Dyson et al.1998; Gaynor et al. 1999) or found dogs to be more at risk (Dodman & Lamb 1992), especially when considering the ASA 1 and 2 categories (Dyson et al.1998).
To the authors’ knowledge, this is the first time that epidural injection of a combination of morphine and bupivacaine has been tested as a risk factor for anaesthetic death. In our study, animals that received an epidural injection showed a statistically not-significant tendency to be more at risk of anaesthetic death. This tendency was unexpected.
The epidural solution of morphine and bupivacaine was prepared as described by Valverde (2008). In this study epidural anaesthesia was performed only by one single veterinarian (CB), thus introducing a potential selection bias. Epidural injections were not equally distributed because they depend on which anaesthetist was on duty and a heavy workload could have led to the absence of epidural injections in patients that would have otherwise received one.
Animals were grouped arbitrarily according to their age in order to obtain four categories as shown in Table 2. It is unlikely that these categories are representative of the metabolic state of the patients. The <3 years old category contained neonates, paediatrics and young adult patients. However, number of subjects enrolled was too low to allow a more detailed classification and an age effect on anaesthetic mortality could have gone undetected.
One team has shown that animals over 12 years old were 7.1 times more at risk of an anaesthetic death when compared to animals of 0.5–8 years old (Brodbelt et al. 2008a). Another study concluded that, in dogs, age was associated with anaesthetic death (Hosgood & Scholl 1998).
Our study did not permit identifying the nature of the procedure as a potential risk factor for anaesthetic death. We chose to classify the nature of the procedure on the basis of its technical description (e.g. examination, soft tissue, orthopaedics), in accordance to earlier publications (Dyson et al. 1998; Hosgood & Scholl 1998, 2002). Other authors have chosen to classify interventions into major or minor procedures (Brodbelt et al. 2007, 2008a). However, there is currently no universally agreed definition of what constitutes a major or a minor procedure. However, it has only been by this classification that procedure has been shown to be to be a risk factor for anaesthetic death in cats and dogs (Brodbelt et al. 2007, 2008a). This is in accordance with the human literature (Wolters et al. 1996; Newland et al. 2002). Studies that have found a significant effect of the nature of the procedure are mainly in large-scale studies including 72,959, 79,178 and 98,036 anaesthetized patients respectively (Newland et al. 2002; Brodbelt et al. 2007, 2008a). In our study, the small number of animals means that a type-II error may have prevented a significant correlation between procedures and death from being shown.
How applicable are our estimates to other veterinary practices? This is an important question because the Centre Hospitalier Ve´te´rinaire des Cordeliers has a different caseload from most practitioners and many of the anaesthetized patients are presented because of the severity of their condition and the necessity for a complex surgical procedure.
Patients of clinical status of ASA 3, 4 and 5 represented 26.6% of our anaesthetized population whereas practice-based studies have shown that 5–10% of the patients were in these categories.
Also, anaesthesia might not be routinely monitored the same way in every practice. This includes the presence of trained staff and/or the use of monitoring devices (electrocardiogram, pulse oximetry, non-invasive or invasive blood pressure monitoring and capnography).
In conclusion, the risk of anaesthetic death appears to be comparable with risk reported internationally. Patients of ASA status 3 and over appear to be considerably more at risk than patients of ASA status 1 and 2. These animals should be thoroughly prepared for anaesthesia and closely monitored by well-trained staff.
References
|